(Link to the original article here) download : Eye rubbing a sine qua non for keratoconus

Eye rubbing as the root cause of keratoconus?
Keratoconus has been labelled a “dystrophy of unknown origin”, and I have long been fascinated by this mysterious disease. A large proportion of my clinical practice is dedicated to the diagnosis, management and prevention of keratoconus, and for many years I have been intrigued by how structural changes and deformation of the corneal wall are so pronounced in keratoconus, yet paradoxically, few detectable genetic and molecular abnormalities exist in this condition.
Eye rubbing has long been acknowledged as a risk factor for keratoconus, but I believe its role in the pathogenesis of keratoconus has not been accorded sufficient prominence. I have thus undertaken the task to pen an article to suggest to readers a pathophysiological concept of keratoconus that I am increasingly convinced of: that eye rubbing is the root cause or sine qua non for keratoconus (article download). As such, eye rubbing is not a « risk factor », as often coined in medical litterature, but the direct cause of a syndrome marked by a corneal deformation labeled « keratoconus ».
In this article, I have put forth the theory that keratoconus is not a dystrophy of unknown genetics and biomolecular substratum, but rather a syndrome caused by eye rubbing. i.e what has been called “keratoconus” is in essence the direct consequence of mechanical trauma to the cornea by chronic and incessant eye rubbing, resulting in the progressive deformation and thinning of the corneal wall which are hallmarks of the disease. Eye rubbing is the main character of the « mechanical » hypothesis as the etiology of keratoconus:
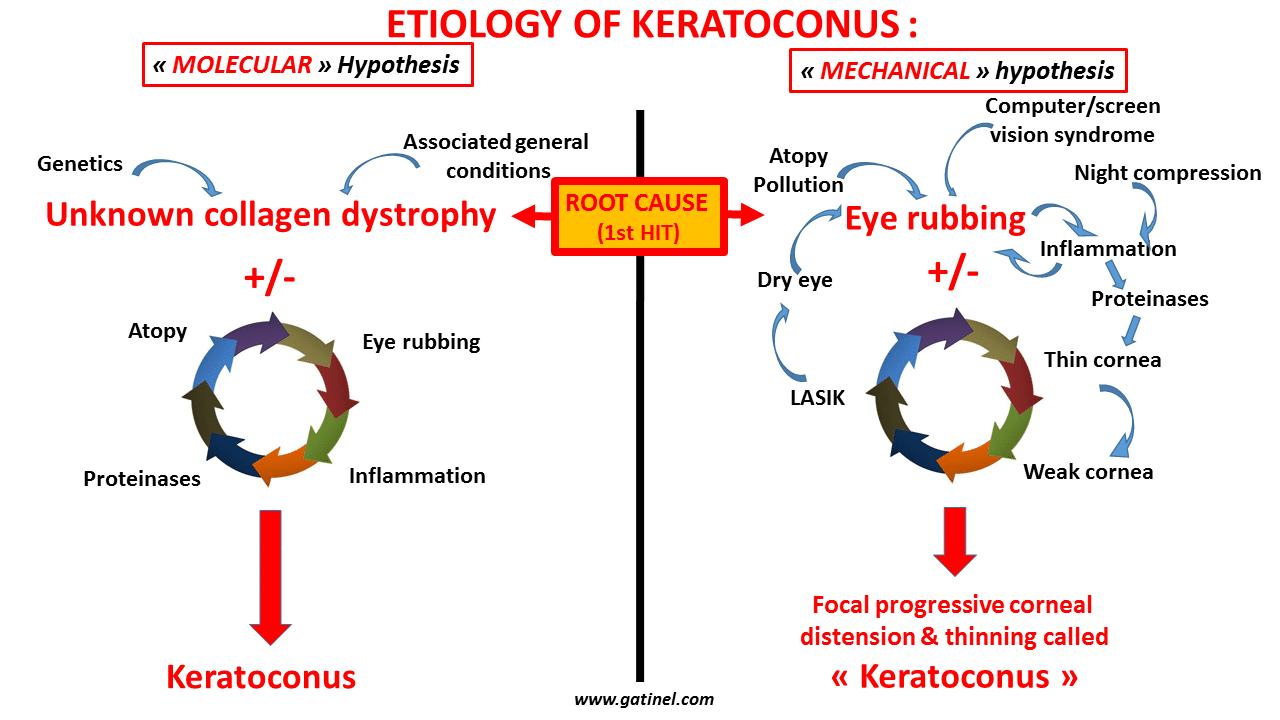
Eye rubbing can cause inflammation. The effect of the mechanical stress (distension) is further accentuated by the release of proteinases in the stroma, explaining the progressive thinning of the cornea, which in turn makes it more vulnerable to the trauma caused by rubbing. LASIK cause eye-dryness, and this can in turn trigger eye rubbing, on a more vulnetable (thinned by the refractive surgery procedure).
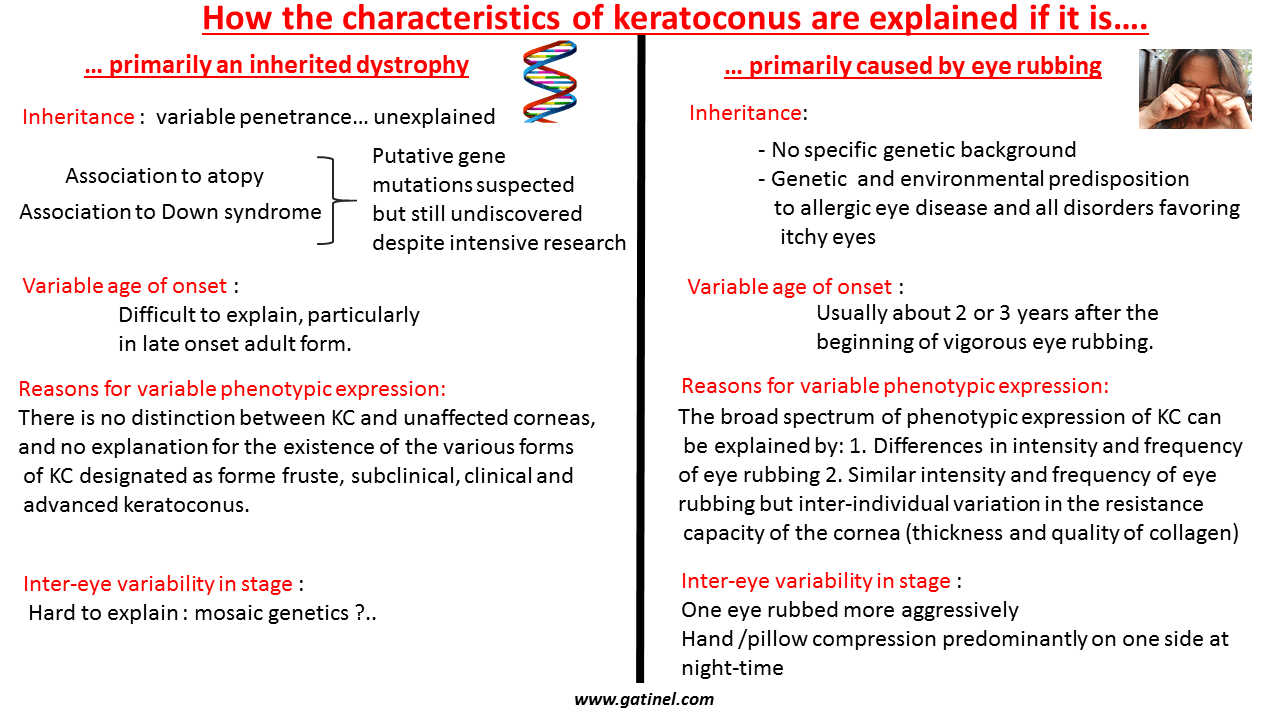
In the Mechanical Hypothesis, keratoconus cannot occur without a repeated mechanical injury such as eye rubbing. When the duration and frequency of eye rubbing exceed the native structural and biomechanical resistance capacity of the cornea, the mechanical imbalance causes the cornea to deform, leading to characteristic topographical patterns, encompassing minor forms of deformation (keratoconus « forme fruste ») to the end stage KC. In my experience, the latter is always encountered in patients who rub the affected eye vigorously and frequently.
Keratoconus as a primary mechanical disease
Just as excessive ligament extension can cause a sprained ankle, chronic eye rubbing can cause the corneal collagen fibers to lose part of their biomechanical resistance, resulting in macroscopically obvious structural deformation. This biomechanical mechanism could also better explain the frequent disparity in the degree of affliction between the right and left eyes (patients frequently rub one eye more often and more vigorously than the other) and the focal nature of keratoconus, which has been recently evidenced.
Marfan syndrome vs Keratoconus
These and other concepts are explored further in the article, through both scientific and anecdotal evidence. A pertinent comparison with the cornea changes in Marfan Syndrome is also made:
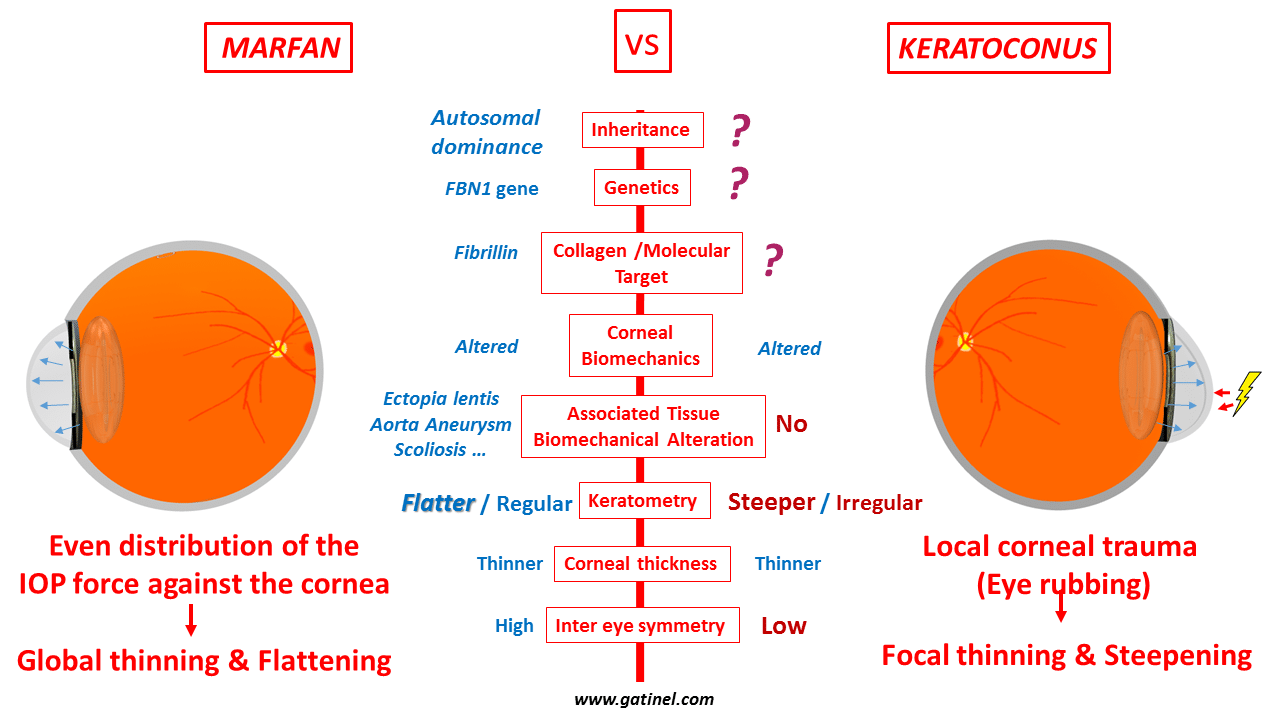
Marfan syndrome represents a perfect counter-example to explain the irrelevance of current theories on the pathogenesis of keratoconus, which describe keratoconus to be an unknown collagen dystrophy associated with environmental, cellular and genetic factors causing a degenerative change in the cornea. In fact, based on these assumptions, Marfan syndrome should perfectly support the theories of keratoconus that attempt to explain the ectatic process. In Marfan syndrome, the gene mutation is identified, and the fibrillin-1 molecule involved in this connective tissue dystrophy is responsible for the reduction of the strength of the collagen present in the ocular tissues, including the corneal stroma. Yet, despite all these features, no keratoconic or ectatatic pattern is seen in the corneas of patients with Marfan syndrome. The Marfan corneas are thinner, but tend to be flatter instead of steeper. This surprising topographical feature can be easily accepted a priori if one considers that in normal conditions, the main force exerted against the cornea is intraocular pressure. Apparatus for measuring pressure within an eye typically include mechanisms to increasingly deform the cornea by applying a progressively increasing force onto it. This force (eg: a puff of air) is responsible of an inward deformation of the corneal surface, which, for the same intraocular pressure, will be easier if the cornea is thinner or biomechanically weaker. Because the force resulting from intraocular pressure is evenly distributed against the posterior surface of the cornea and the inner surface of the sclera, a softer eyeball will undergo a progressive distension of its shell, which causes the local radii of curvature of the cornea to increase (and the corneal curvature to decrease), with concomitant progressive thinning. Hence, in the absence of a localized or focal additional force or trauma, the biomechanical weakening of Marfan corneas results in a flatter corneal surface. This distension of the eyeball also contributes to its increase in axial length, and most Marfan patients indeed suffer from axial myopia . Abnormally flat corneas and axial myopia both correspond to the ocular diagnostic criteria for Marfan syndrome.
Although a flat keratometry is a diagnostic criteria for a Marfan cornea, some association between Marfan syndrome and keratoconus has been reported. This however does not contradict the mechanical theory: the biomechanically weaker corneas of Marfan patients may be more vulnerable to the effects of eye rubbing.
In contrast to the Marfan cornea, the typical topographic pattern of a keratoconus cornea includes steepening and asymmetry of the corneal surface and changes in the corneal thickness, including central or paracentral accelerated thinning. Invoking an external source of trauma to the cornea (such as eye rubbing) as a pathogenetic cause provides a better explanation to these findings than still unraveled processes of molecule change mysteriously affecting only the cornea and preserving the other tissue components of the body. The force exerted against the corneal shell by the pressure of the fingers, particularly the knuckles, may be considerable. Repetitive force can cause stretching and disorganization of the corneal collagen lamellae. An acute rise in intraocular pressure from sudden reduction in eye volume from the compression of the globe by the fingers could also stretch the scleral shell and lead to an axial myopic refractive shift. Despite contradicting reports, the axial length of keratoconus patients seems to be slightly but significantly higher than in non-keratoconus patients.
There will understandably be skeptics and naysayers to this theory, especially since the hypothesis may be impossible to prove. However, the primary purpose of this article is to increase the awareness of the potential ill-effects of eye rubbing and its association with keratoconus. Highlighting its causative role may help to dramatically reduce the incidence of keratoconus, and stop its progression in eyes already affected.
It is interesting to note that conditions that are characterized by the presence of corneal inflammation generally induce a reduction in corneal curvature, not an increase in corneal curvature. This also underlines the importance of the mechanical hypothesis to account for the focal steepening which is observed in corneas with keratoconus.
In conclusion:
The “eye rubbing as a sine qua non for keratoconus” theory blatantly defies the widely accepted concept of keratoconus being a corneal dystrophy of unknown origin. To many, it may appear provocative in its simplicity, and on a personal level, would have triggered some skepticism 6 or 7 years ago. However, in recent years, after conceiving the hypothesis and applying it to my day to day management of keratoconus patients, the skepticism is waning. The theory is compatible with most of what is known about keratoconus. In fact, day by day, after each patient interview, I am increasingly convinced that this mechanical first hit theory is the answer to the enigma surrounding keratoconus. This opens fascinating perspectives. It could close the chapter of the mystery of the pathogenesis of keratoconus opened by Dr John Nottingham’s 1854 treatise on the conical cornea. In theory, it could also lead to the eradication the disease if it were possible to prohibit everyone from chronically and incessantly rubbing their eyes. However, from a practical standpoint, this is probably an impossible mission.
A less ambitious but important goal is still attainable, and this involves reducing the incidence and progression of keratoconus by increasing the awareness of patients on the potential dangers of chronic and vigorous eye rubbing, and encouraging them to refrain from it. In the management of my many patients with keratoconus, I religiously counsel them on the dangers of eye rubbing, and tell all of them to stop rubbing their eyes. I also routinely perform detailed evaluation of their condition, including refraction and subtractive topography maps between each consultation to document disease progression. None of my patients who have completely stopped rubbing their eyes have seen progression in their disease since they kicked the habit. These observations are still ongoing, and will require a longer follow-up, but if they stand the test of time, they will bring forth a strong argument to support the “eye rubbing as a sine qua non for keratoconus’ theory, and more importantly, demonstrate its clinical benefits.